If you have spent any time researching anti-ageing supplements in Malaysia, you have likely been caught in a tug-of-war. One Instagram clinic in Mont Kiara promises a NAD+ infusion that “resets your cells in 90 minutes”. A US podcast insists nicotinamide riboside, sold as Tru Niagen, is the only molecule with real human data.
A Shopee listing claims its liposomal NMN is “six times more bioavailable” than capsules. And somewhere in the comment section, an uncle is asking why nobody just takes a RM12 bottle of niacin from Watsons.
The choice is genuinely confusing, the marketing is loud, and the published evidence is quieter than any of the sellers will admit. Here are the mechanisms, the human trials, the prices in Malaysian ringgit, and the stacks the longevity influencers are pushing. By the end you should have a clear, honest framework for deciding what - if anything - to buy.
For the underlying biology of NAD+ itself, see our science section. For the symptom-level outcomes you might be hoping for, see benefits. For specific products on shelves locally, see brands. And if you are weighing an IV drip versus a capsule, the local clinics section lists what is actually on offer in Klang Valley, Penang and Johor Bahru.
The mechanism question: are NMN and NR really different?
NAD+ is the cellular currency that powers sirtuins, DNA-repair enzymes, and mitochondrial respiration. Levels fall with age, and a large body of preclinical work suggests restoring them produces measurable benefits in mice (Mills et al., 2016). The question is how to restore them in humans.
There are four practical oral precursors: tryptophan, niacin (nicotinic acid), nicotinamide (NAM), nicotinamide riboside (NR), and nicotinamide mononucleotide (NMN). All converge on NAD+ through overlapping salvage pathways (Rajman et al., 2018).
The marketing distinction usually goes like this: NMN is “one step closer” to NAD+ than NR, because NR must first be phosphorylated to NMN before becoming NAD+. Therefore, the argument runs, NMN is more efficient.
The problem with this story is that conversion happens inside the cell anyway, the enzymes are abundant, and the rate-limiting step in most tissues is not that single phosphorylation. The Charles Brenner camp argues NR is the more validated molecule because it has the larger published human trial portfolio. The Shin-ichiro Imai and Leonard Guarente camp argues NMN is more direct and possibly bypasses age-related declines in the NRK enzymes (Imai & Guarente, 2014).
Both camps have skin in the commercial game. As a Malaysian buyer, you should treat the “which is better” debate as unsettled.
What we can say with confidence: both molecules raise blood NAD+ in human studies. NR has been shown to do so reliably in the Trammell trial and several follow-ups (Trammell et al., 2016). NMN has shown comparable effects in Japanese men, Japanese postmenopausal women (Yoshino et al., 2021), older Japanese adults (Igarashi et al., 2022), and amateur runners (Liao et al., 2021).
What we cannot say is that one outperforms the other on any clinical endpoint, because no adequately powered head-to-head human trial has been published (Yoshino & Imai, 2018).
NAD+ IV therapy: the expensive cousin
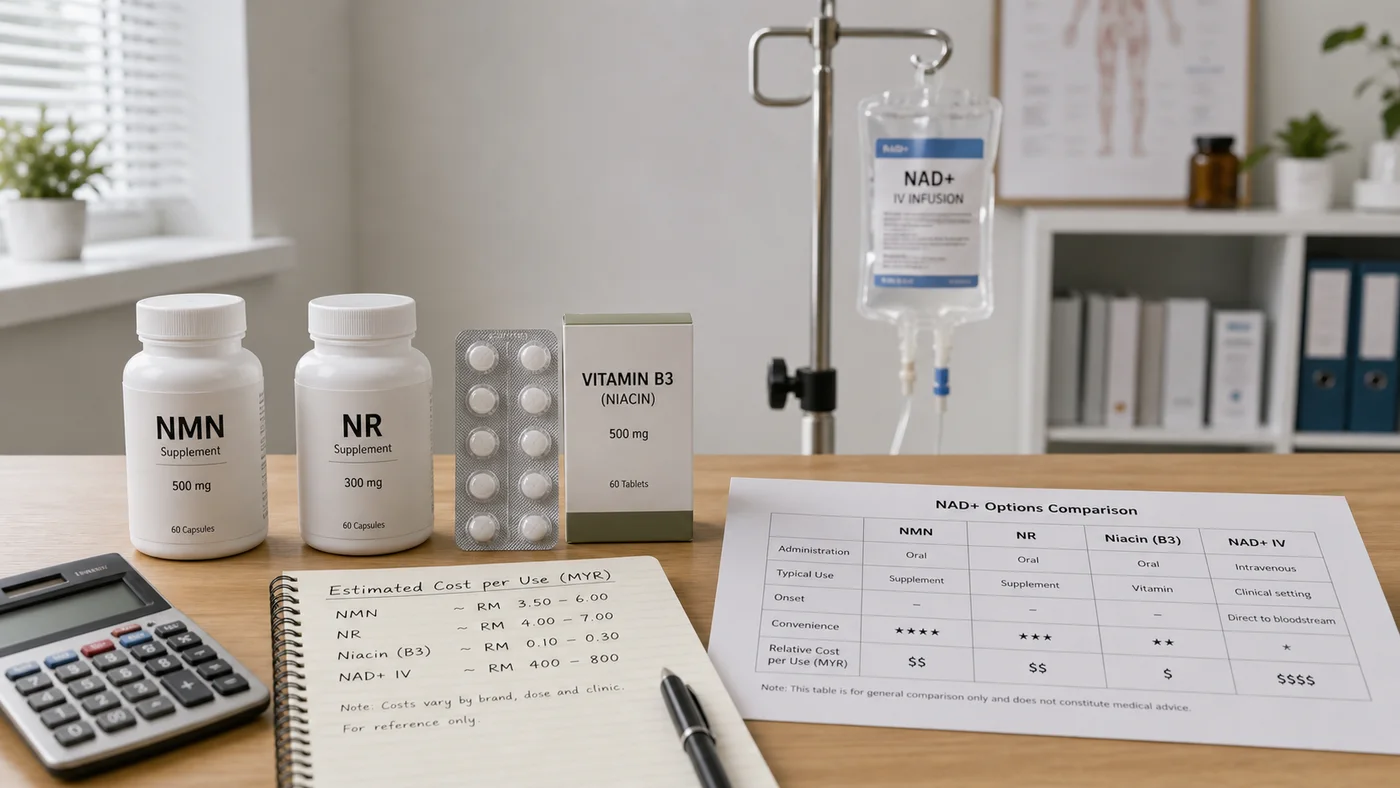
NAD+ intravenous therapy is the most aggressive option marketed in Malaysia. Several aesthetic and “wellness” clinics in Bangsar, Mont Kiara, Damansara Heights and Penang offer drips ranging from 250 mg to 1,000 mg per session, typically priced between RM800 and RM2,500. Some packages bundle in glutathione or vitamin cocktails to justify the bill.
The pitch is straightforward: bypass digestion, deliver NAD+ directly to the bloodstream, get faster results. The evidence is much thinner than the pitch.
Peer-reviewed human trials of intravenous NAD+ are sparse, generally small, and have not demonstrated clinical superiority over oral precursors taken consistently (Verdin, 2015). Patients frequently report flushing, chest pressure and nausea during infusion, which is why clinics drip slowly over 60–120 minutes.
There is also a regulatory point. The National Pharmaceutical Regulatory Agency (NPRA) does not register NAD+ as a therapeutic indication for healthy ageing, and intravenous compounding is governed by separate clinical standards. If you are paying RM2,000 for a drip, you are paying for clinic overhead and the perceived sophistication of the needle, not for evidence the needle does more than a capsule.
For most healthy Malaysian adults, IV NAD+ is the worst value option. We are not saying it does nothing - only that the cost-to-evidence ratio is poor.
The cheap end: niacin and nicotinamide
Walk into any Watsons, Caring or Guardian and you can buy niacin (vitamin B3) or nicotinamide tablets for under RM30. Both raise NAD+ effectively. So why is anyone paying ten times more for NMN?
Two real reasons. First, niacin at NAD+-relevant doses causes vasodilation - the famous “niacin flush” - which is uncomfortable enough that most people quit within a week. Slow-release formulations reduce flushing but introduce hepatotoxicity risk at high doses.
Second, both niacin and nicotinamide are processed through methylation pathways. Chronic high doses can deplete the body’s methyl donors, with downstream implications for homocysteine and other markers.
That said, for a Malaysian buyer on a tight budget who is methylation-aware (taking adequate folate and B12) and tolerates flushing, niacin remains a defensible option. It is honest to admit this, even if it undercuts the entire premium NMN market.
Price-per-gram in Malaysian ringgit
Let us put the options on the same scale. Prices below are typical 2026 ranges in Malaysia, including import duty and shipping where relevant.
- Niacin or nicotinamide (Watsons, generic): roughly RM0.05–RM0.15 per gram. Effectively free.
- NR (Tru Niagen, Chromadex licensee, imported): roughly RM5–RM9 per gram, sold as 300 mg capsules at around RM200–RM350 for a 30-day supply.
- NMN (mid-tier Malaysian or Singaporean brand, third-party tested): roughly RM4–RM8 per gram, sold as 250–500 mg capsules at RM200–RM500 per month.
- NMN (premium imported, 99%+ purity claims): roughly RM10–RM20 per gram.
- NAD+ IV therapy: at 500 mg per session and RM1,500 per session, that is RM3,000 per gram of NAD+ delivered.
The ranking by value is consistent: niacin > generic nicotinamide > mid-tier NMN ≈ NR > premium NMN >> IV. The ranking by evidence is roughly: NR ≈ NMN > niacin/nicotinamide > IV. The ranking by tolerability and convenience is: NMN ≈ NR > nicotinamide > niacin > IV.
Most readers will land on either NR or mid-tier NMN as the rational compromise.
Liposomal, sublingual, capsule: does delivery matter?
Brands love to charge a premium for “advanced delivery”. The three main formats are standard capsules, sublingual tablets or powders (held under the tongue), and liposomal preparations (NMN encapsulated in phospholipids).
Here is the honest picture. NMN is a relatively small, water-soluble molecule with reasonable oral bioavailability already. Sublingual delivery may bypass first-pass metabolism for some fraction of the dose, but published comparisons in humans are thin and often industry-funded. Liposomal claims usually rest on in-vitro permeability data, not on clinical pharmacokinetic head-to-heads.
Our practical advice: pay for purity and third-party testing, not for delivery format. If a capsule with a Certificate of Analysis costs half as much as a liposomal version with vague claims, the capsule is the better buy.
The popular stacks: NMN with resveratrol, metformin, CoQ10, rapamycin
NMN with resveratrol. Popularised by Professor David Sinclair, who has commercial interests in companies selling these molecules. The biological rationale is mechanistically tidy. The human evidence for synergy is weaker than the rationale suggests.
NMN with metformin. Metformin is a prescription diabetes drug being studied for longevity (the TAME trial). Some clinicians prescribe it off-label to non-diabetics in Malaysia; this is a grey zone. Importantly, metformin may blunt some exercise-induced NAD+ adaptations in muscle.
NMN with CoQ10. Different mechanisms. They are complementary rather than redundant, and there is no known antagonism. A reasonable stack for adults over 50, particularly those on statins.
NMN with rapamycin. Rapamycin is prescription-only in Malaysia and tightly controlled. It is not a self-directed option.
How to actually decide
If you are a healthy Malaysian adult considering an NAD+ precursor for the first time, here is a defensible decision tree.
Start by asking what problem you are solving. If the honest answer is “I read a Twitter thread”, pause. If it is “I have measurable energy decline, my sleep is poor, I am over 45, I exercise regularly and want to support recovery” - that is a reasonable case for trialling an oral precursor.
Next, set a budget. If RM200 per month is the ceiling, choose between mid-tier NMN, NR, or generic nicotinamide. If RM50 is the ceiling, niacin or nicotinamide is the only honest answer. If budget is not a constraint, mid-tier NMN with a Certificate of Analysis is a sensible default - premium pricing rarely buys premium evidence.
Third, set a trial period and measure something. Eight to twelve weeks. Track sleep, perceived energy, exercise recovery, and if possible a basic blood panel before and after. If nothing changes, stop.
Finally, avoid the IV unless a physician has a specific reason.
Tropical climate considerations across formats
The Malaysian climate adds a wrinkle international comparisons often miss. Loose powder and liquid liposomal formats degrade fastest in heat and humidity. Sublingual tablets can clump within weeks of opening. Standard capsules in airtight HDPE bottles with desiccant remain the most stable choice for ambient Malaysian storage.
This makes the format comparison practical, not theoretical. A premium liposomal NMN that requires fridge storage and which loses potency if you forget to refrigerate it after a long workday is a worse practical choice than a stable mid-tier capsule, regardless of the in-vitro absorption claims. Buy what you can store consistently.
Long-term cost-per-year math in MYR
Run actual numbers across a 12-month commitment at a 500mg/day target:
- Mid-tier NMN at RM 4/gram (verified Shopee Mall): roughly RM 730/year
- Premium imported NMN at RM 12/gram (brand-direct plus SST): roughly RM 2,190/year
- NR Tru Niagen at RM 7/gram equivalent (300mg/day): roughly RM 770/year
- Generic niacin from Watsons: RM 30-50/year
- Weekly NAD+ IV (52 sessions × RM 1,500): RM 78,000/year
- NMN + resveratrol Sinclair stack (both premium): RM 3,500-4,500/year
For most Malaysian middle-income buyers, mid-tier NMN or NR is the rational landing point. Niacin remains the defensible budget pick for flushing-tolerant readers. Weekly NAD+ IV is a poor cost-evidence ratio.
Bottom line for Malaysian buyers
NMN and NR are roughly equivalent on current human evidence. Both raise NAD+. Neither has been proven clinically superior.
Niacin and nicotinamide are cheap and work, with tolerability trade-offs. NAD+ IV therapy is overpriced relative to its evidence. Liposomal and sublingual claims are mostly marketing. Stacks make sense in moderation, with eyes open about who is selling them.
Pick the option whose price, format and brand transparency you can defend to a sceptical friend. If you cannot defend it to that friend, you are buying marketing, not biology.
Open questions we will revisit
The field is moving quickly. Several open questions we expect to resolve in the next 2-5 years and that will change this guide:
Will adequately powered head-to-head NMN-vs-NR human trials emerge? Several phase-2 trials in flight will resolve direct clinical comparisons. Update expected after publication.
Does Slc12a8 turn out to be a real human NMN transporter? Replication efforts continue. If confirmed, this supports the Imai camp and shifts the NMN-vs-NR marketing balance.
Does NAD+ IV show stronger clinical effect in defined populations (post-surgical recovery, addiction recovery)? Better-designed trials may justify IV use for specific indications, even if not for general healthy ageing.
Does long-duration low-dose NMN (250mg/day for years) show cumulative effects? No such trial exists. Long-term users are an informal observational cohort.
Article version 2026-04 - first published 2026-04-26; the last-updated date is shown at the top. Reviewed by T Dinaiz. Comparisons here use 2026 Malaysian retail pricing; expect price-per-gram updates as the local market matures and as the SGD/USD rates shift.
For readers paralysed by the choice, the most defensible starting move is the cheapest option you can tolerate: niacin at RM 12 per month for one to two months, with attention to flushing and a baseline blood panel. If you tolerate flushing, niacin essentially answers the question for far less spend than premium NMN. If flushing is intolerable, mid-tier NMN is the next practical step.